FRONTIERS IN MEDICAL CASE REPORTS - Volume 7; Issue 3, (May-Jun, 2026)
Pages: 01-10
Print Article
Download XML Download PDF
Acute Left Parietal and Occipital Cortical Infarcts Secondary to Severe Left Internal Carotid Artery Stenosis: A Case Report
Author: Mayesha Ahmed, Madyson FitzGerald, Abeera Rabbani, Roxana Lazarescu
Category: Medical Case Reports
Abstract:
Severe internal carotid artery (ICA) stenosis is an important and treatable cause of ischemic stroke, but diagnosis can be challenging when presentation is confounded by seizure activity and postictal neurological deficits. We report the case of a 77-year-old man with a history of prior cerebrovascular accidents, dementia, and seizure disorder who presented with multiple witnessed seizures followed by slurred speech, right facial droop, and right-sided weakness. Initial CT of the head showed only chronic ischemic changes, while CT angiography revealed severe (70–99%) stenosis of the left cervical ICA. Because of active seizures and concern for Todd’s paralysis, thrombolysis was deferred. EEG demonstrated epileptiform discharges over the left hemisphere, and although the patient showed rapid clinical improvement, MRI of the brain later revealed acute left parietal and occipital cortical infarcts with a subacute left corona radiata infarct. The infarct distribution was consistent with an artery-to-artery embolic pattern, and the ipsilateral high-grade ICA stenosis was considered the most likely contributing source, although a cardioembolic etiology could not be excluded in the setting of a known patent foramen ovale and multiple prior cerebrovascular events. The patient was managed medically with levetiracetam, dual antiplatelet therapy, and statin therapy, as he was not a candidate for carotid intervention given his advanced dementia and poor functional status. This case illustrates that acute ischemic stroke may coexist with postictal deficits and may be missed on initial imaging. In patients with high-grade carotid stenosis and a clinically ambiguous presentation, advanced neuroimaging and systematic etiologic evaluation are essential for accurate diagnosis and individualized management.
Keywords: Ischemic Stroke, Internal Carotid Artery Stenosis, Large Vessel Atherosclerosis, Artery-To-Artery Embolism and Todd’s Paralysis
DOI URL: https://dx.doi.org/10.47746/FMCR.2026.7304
Full Text:
Introduction
Ischemic stroke remains a leading cause of morbidity and mortality worldwide, accounting for the majority of cerebrovascular events (GBD Stroke Collaborators, 2021; Campbell and Khatri, 2020). It results from an interruption of cerebral blood flow, most commonly due to thromboembolic occlusion of intracranial or extracranial vessels, leading to focal neurological deficits (Campbell and Khatri, 2020). Among the diverse etiologies, large vessel atherosclerosis plays a critical role, particularly in the setting of high-grade stenosis of the internal carotid artery (ICA) (Kleindorfer et al., 2021). Atherosclerotic plaque formation at the carotid bifurcation and proximal ICA can lead to artery-to-artery embolization or hemodynamic compromise, both of which contribute to cerebral infarction (Kleindorfer et al., 2021). Patients with severe ICA stenosis are at especially high risk for recurrent ischemic events, even when managed with optimal medical therapy (Kleindorfer et al., 2021).
Cortical infarcts involving the parietal and occipital lobes are of particular clinical importance due to their variable and sometimes subtle presentations (Caplan and Hennerici, 1998). Infarction in these regions may manifest with higher-order neurological deficits, including aphasia, visuospatial impairment, or visual field deficits, and can occasionally be misattributed to alternative diagnoses such as postictal states (Caplan and Hennerici, 1998; Feldman and Gidal, 2013). Furthermore, involvement of multiple vascular territories, including the posterior cerebral artery distribution, may raise concern for embolic phenomena and complicate diagnostic evaluation by necessitating differentiation between artery-to-artery and cardioembolic sources (Hart et al., 2014).
We present a complex case of a 77-year-old male with multiple vascular risk factors and prior cerebrovascular disease who presented with recurrent seizures and acute focal neurological deficits in the setting of severe left ICA stenosis. This case highlights several clinically significant challenges, including the differentiation between acute ischemic stroke and postictal neurological deficits (Feldman and Gidal, 2013), the identification of an artery-to-artery embolic pattern involving both anterior and posterior circulation territories (Hart et al., 2014), and the limitations of therapeutic options in patients who are not candidates for surgical or endovascular intervention (Kleindorfer et al., 2021). Additionally, it underscores the need for individualized management strategies in patients with recurrent ischemic events despite guideline-directed medical therapy (Kleindorfer et al., 2021), as well as the importance of integrating clinical, radiographic, and electroencephalographic data in complex neurovascular presentations.
Case Presentation
This case presents a 77-year-old male with a past medical history of multiple prior cerebrovascular accidents, hypertension, hyperlipidemia, dementia, prior transient ischemic attack, and seizure disorder. He was brought to the emergency department from a nursing facility after experiencing approximately six witnessed seizure episodes within one hour prior to arrival.
On arrival, the patient exhibited acute neurological deficits, including slurred speech, right-sided facial droop, and right-sided weakness. Nursing facility staff reported that the focal deficits were observed immediately following the seizure cluster, though the precise interval between seizure onset and the appearance of neurological symptoms could not be established from available history. His last known well time was approximately 17:30. A stroke alert was activated. Initial vital signs were within normal limits. Neurological examination revealed altered mental status with impaired orientation, incoherent speech, mild-to-moderate aphasia, dysarthria, and right-sided motor deficits. The initial National Institutes of Health Stroke Scale (NIHSS) score was 6–7, consistent with a moderate stroke.
Non-contrast CT of the head demonstrated chronic ischemic changes, including periventricular white matter disease and old lacunar infarcts in the left caudate head, corona radiata, and centrum semiovale, without evidence of acute hemorrhage (Fig. 1). CT and CTA were performed within approximately one hour of ED arrival.
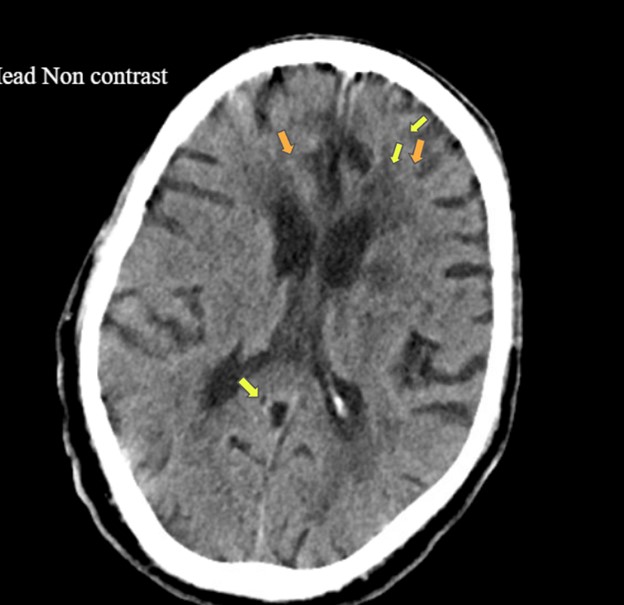
Figure 1: Non-contrast CT of the head shows chronic periventricular white matter hypodensities and lacunar infarcts, consistent with longstanding small vessel ischemic disease, without acute hemorrhage.
Orange arrows: Periventricular hypodensities consistent with chronic small vessel ischemic disease
Yellow arrows: Chronic lacunar infarcts in the left deep white matter (caudate/corona radiata region)
CT angiography of the head and neck revealed high-grade stenosis of 70–99% of the left cervical internal carotid artery (ICA) due to non-calcified plaque at the carotid bulb and proximal ICA. No large vessel occlusion, aneurysm, or dissection was identified (Fig. 2).

Figure 2: CT angiography of the head and neck demonstrates high-grade stenosis of the left internal carotid artery at the carotid bulb.
Green arrow: High-grade stenosis of the proximal left internal carotid artery at the carotid bulb
Given the presence of active seizures and concern for postictal neurological deficits, intravenous thrombolysis was deferred. The patient was treated with a loading dose of 3 grams intravenous levetiracetam, followed by maintenance dosing of 1 g twice daily, and admitted for further stroke and seizure evaluation. He was continued on dual antiplatelet therapy of aspirin and clopidogrel and high-intensity statin therapy.
Electroencephalography, which was performed within a few hours of arrival, demonstrated epileptiform discharges over the left hemisphere with focal slowing, consistent with underlying cerebral dysfunction (Fig. 3). Over the next 24 hours, the patient showed marked clinical improvement, with near-complete resolution of motor deficits and reduction in NIHSS to 2 on serial neurological examination. This suggested a component of postictal paralysis or Todd’s paralysis. MRI of the brain, including diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) sequences, was obtained approximately 18 hours after presentation.
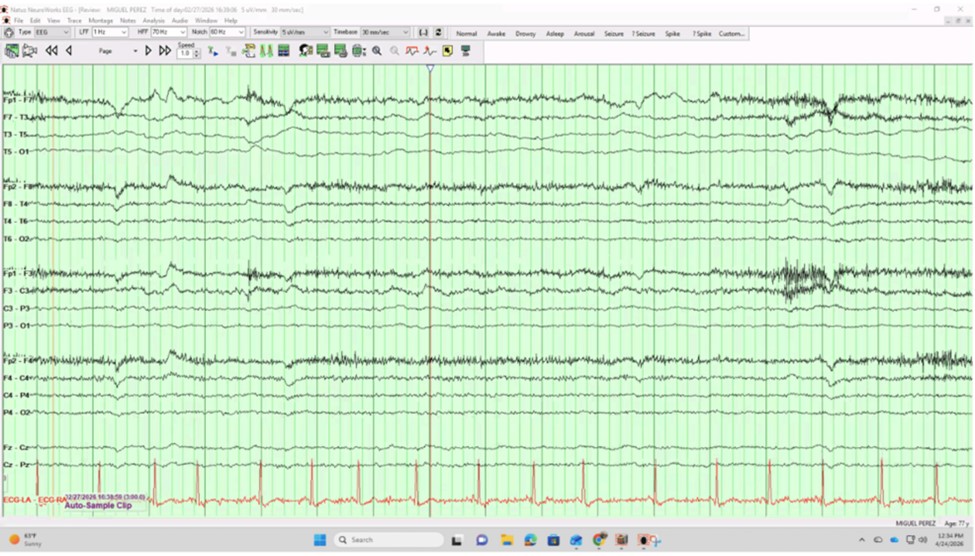
Figure 3: EEG recording demonstrating predominantly normal background activity with intermittent right temporal sharp/fast discharges. Frontal slow-wave deflections are consistent with eye movement artifact. The bottom red channel represents ECG, showing regular cardiac rhythm.
Black traces = EEG channels (cortical electrical activity)
Red trace = ECG (heart rhythm)
Sharp spikes = Possible epileptiform discharges
Smooth rhythmic waves = Background activity
Large slow deflections (frontal) = Likely eye movement artifact
Subsequent MRI of the brain revealed several punctate acute infarcts in the left parietal and left occipital cortical regions, along with a subacute infarct in the left corona radiata (Fig. 4). The infarct distribution was felt to be most consistent with an artery-to-artery embolic pattern, with the ipsilateral severely stenotic left ICA considered the most probable contributing source. However, a cardioembolic mechanism could not be excluded, particularly given the presence of a patent foramen ovale, multiple prior cerebrovascular events, and involvement of the posterior cerebral artery territory. The cardiac monitoring performed during this admission consisted of continuous telemetry; no prolonged ambulatory monitoring was completed, and transesophageal echocardiography was not performed, which limits the completeness of the cardioembolic workup.
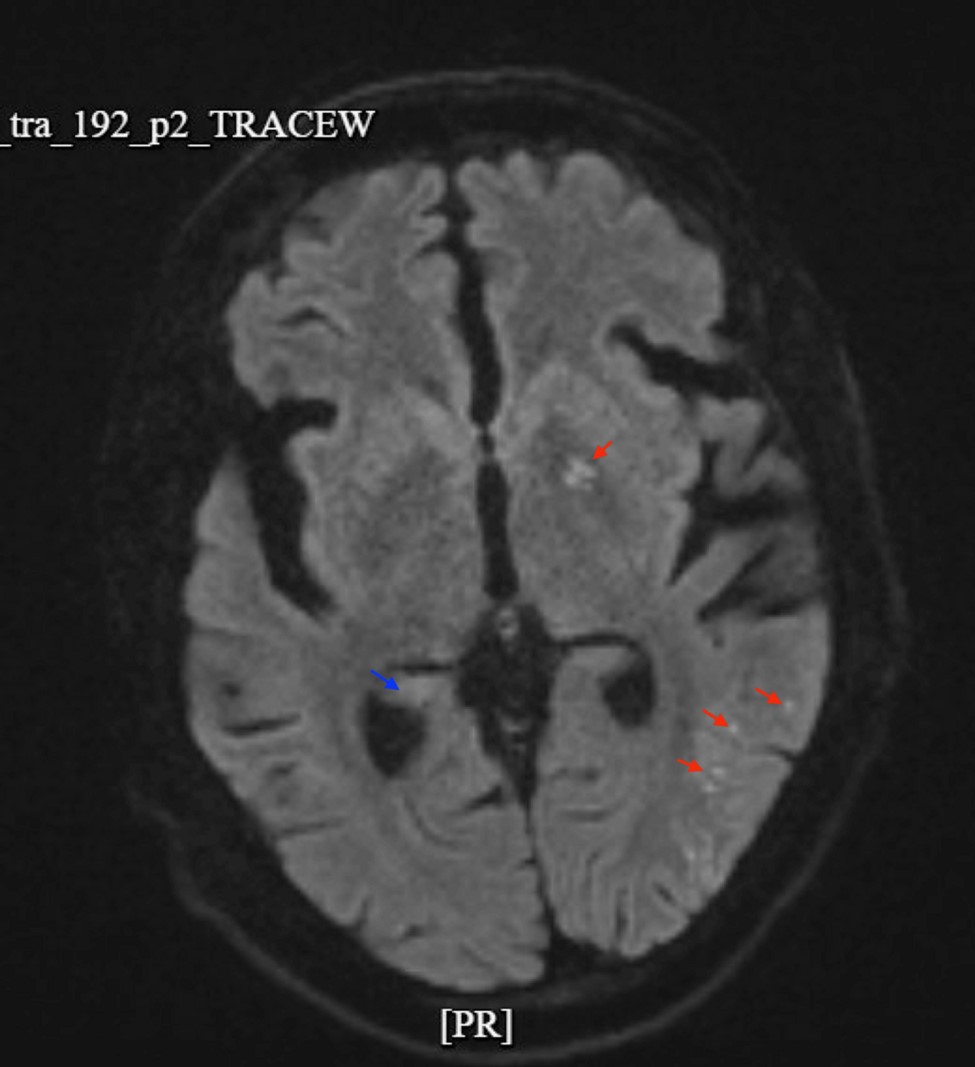
Figure 4: Diffusion-weighted MRI (bottom) reveals multiple punctate foci of restricted diffusion in the left cerebral hemisphere (red arrows), as well as a lesion in the left corona radiata, consistent with acute and subacute infarcts.
Red arrows: Acute punctate cortical infarcts in the left parietal and occipital lobes;
Blue arrow: Subacute infarct in the left corona radiata
Further evaluation showed normal glycemic control with HbA1c of 5.2% and well-controlled lipid levels with LDL 60 mg/dL. Lipoprotein(a) was slightly elevated. Cardiac monitoring did not reveal atrial fibrillation. Prior transthoracic echocardiography demonstrated preserved ejection fraction with a patent foramen ovale.
Vascular surgery consultation had previously determined that the patient was not a suitable candidate for carotid intervention due to advanced dementia, poor baseline functional status, and high perioperative risk. Electrophysiology consultation for implantable loop recorder placement was declined by the patient’s family.
The patient was managed conservatively with antiepileptic therapy, dual antiplatelet therapy, and statin therapy. Given the occurrence of recurrent ischemic events despite dual antiplatelet therapy, alternative antithrombotic strategies were briefly considered; however, no change was made in the absence of a confirmed cardioembolic source and given the uncertainty of benefit in this clinical context. At the time of discharge planning, the patient had returned close to his neurological baseline, with persistent mild cognitive impairment consistent with prior dementia.
Discussion
This case illustrates a complex presentation of acute ischemic stroke in the setting of severe (70–99%) left internal carotid artery (ICA) stenosis, complicated by concurrent seizure activity and transient postictal neurological deficits. The patient’s clinical course highlights important diagnostic and therapeutic challenges, particularly in distinguishing acute stroke from postictal phenomena and in managing recurrent ischemia despite optimal medical therapy.
Severe ICA stenosis is a well-established cause of ischemic stroke through an artery-to-artery embolic mechanism, in which unstable atherosclerotic plaque at the carotid bifurcation generates emboli that travel distally into cortical branches of the middle and posterior cerebral arteries. Cortical infarcts involving the parietal and occipital lobes, as seen in this patient, may be consistent with embolic phenomena rather than small vessel disease. The presence of non-calcified plaque on CTA raises the possibility of plaque vulnerability, which has been associated with a higher risk of embolization and recurrent stroke (North American Symptomatic Carotid Endarterectomy Trial Collaborators, 1991). That said, the available vascular imaging does not exclude competing mechanisms, and the diagnosis of carotid plaque embolism as the primary etiology should be understood as the most probable explanation given the available data, rather than a confirmed causal attribution.
Although ICA disease classically affects anterior circulation territories, emboli may reach the posterior cerebral artery via collateral pathways, including a fetal posterior cerebral artery configuration or leptomeningeal anastomoses. This may offer one explanation for the involvement of the occipital cortex in this case, though it does not exclude a cardioembolic source for this territory. Similar patterns of infarction have been described in patients with high-grade carotid stenosis and are compatible with an artery-to-artery embolic mechanism (Fisher and Engel, 2010), but anatomic proximity alone is insufficient to confirm the embolic source, particularly in patients with concurrent structural cardiac abnormalities such as a PFO.
A key diagnostic challenge in this case was differentiating acute ischemic stroke from postictal (Todd’s) paralysis, particularly given the patient’s history of seizures and the occurrence of multiple seizure episodes prior to presentation. Todd’s paralysis is a transient focal neurological deficit that can mimic stroke and typically resolves within 48 hours (Powers et al., 2019). In this patient, the rapid improvement in motor deficits and NIHSS score initially supported a postictal etiology. However, subsequent MRI revealed acute cortical infarcts, confirming that both processes—seizure-related deficits and true ischemic injury—coexisted. This underscores the importance of advanced neuroimaging in patients with ambiguous presentations, as reliance on clinical improvement alone may lead to underdiagnosis of acute infarction.
The management of acute ischemic stroke in the setting of active seizures is controversial. Current guidelines consider seizure at onset a relative contraindication to intravenous thrombolysis unless there is clear evidence of a persistent neurological deficit attributable to stroke rather than postictal state (Powers et al., 2019). In this case, thrombolysis was deferred due to ongoing seizures and diagnostic uncertainty, which is consistent with guideline-based practice.
Another important aspect of this case is the occurrence of ischemic stroke despite dual antiplatelet therapy (DAPT) and high-intensity statin use, indicating treatment failure and high residual vascular risk. While DAPT is recommended for short-term secondary prevention after minor stroke or high-risk transient ischemic attack, long-term management typically involves single antiplatelet therapy due to bleeding risk (Powers et al., 2019). The recurrence of ischemic events in this patient raises the question of whether alternative strategies—such as anticoagulation or modification of antiplatelet regimens—might reduce further risk. However, evidence supporting such approaches in patients with non-cardioembolic stroke and competing stroke mechanisms remains limited, and any change in antithrombotic regimen would require a clearer characterization of the dominant stroke mechanism and careful individualized risk-benefit assessment.
Carotid revascularization, including carotid endarterectomy (CEA) or carotid artery stenting (CAS), is strongly recommended for symptomatic patients with 70–99% ICA stenosis, as it significantly reduces the risk of recurrent stroke (Brott et al., 2011). However, patient selection is critical. In this case, the decision to forgo intervention reflected a patient-specific assessment of risk and goals of care: the patient’s advanced dementia, limited functional status, and high perioperative risk rendered him a poor candidate in the judgment of the vascular surgery team. This should not be interpreted as a general limitation of guideline-directed therapy; rather, it illustrates how standard treatment recommendations must be adapted to individual clinical circumstances, particularly when baseline function and life expectancy significantly alter the risk-benefit calculus.
The presence of a patent foramen ovale (PFO) introduces an additional potential embolic source that warrants acknowledgment. In this case, the workup for cardioembolism was incomplete: transthoracic echocardiography demonstrated the PFO but transesophageal echocardiography was not performed, prolonged cardiac monitoring was not obtained, and no venous thromboembolism evaluation was documented. These gaps limit the confidence with which cardioembolism can be excluded. A cardioembolic etiology was considered less likely given the anatomical presence of high-grade ipsilateral carotid stenosis, but this inference rests on probabilistic reasoning rather than definitive exclusion. Current evidence suggests that PFO closure is most beneficial in younger patients with cryptogenic stroke, and its role in elderly patients with competing stroke mechanisms is uncertain (Saver et al., 2017).
Finally, this case highlights the interplay between post-stroke epilepsy and recurrent cerebrovascular events. Seizures are a known complication of cortical infarcts and may both mimic and exacerbate neurological deficits (Beghi et al., 2011). The presence of epileptiform discharges on EEG and the clinical response to levetiracetam support a diagnosis of post-stroke epilepsy, which requires ongoing management to prevent further episodes and diagnostic confusion.
Conclusion
In patients with high-grade carotid stenosis and a clinically ambiguous presentation, physicians should maintain a low threshold for pursuing advanced neuroimaging, such as MRI with diffusion-weighted sequences, to detect infarction that may be missed on initial CT. A thorough and systematic etiologic evaluation—including adequate cardiac monitoring and echocardiography—is important to characterize the stroke mechanism and guide management, particularly when structural cardiac abnormalities such as a PFO are present. Early recognition of symptomatic severe ICA stenosis and individualized treatment planning, whether through intervention when appropriate or optimized medical therapy, remain the cornerstones of secondary stroke prevention.
References:
Beghi E, D'Alessandro R, Beretta S, Consoli D, Crespi V, Delaj L, Gandolfo C, Greco G, La Neve A, Manfredi M, Mattana F, Musolino R, Provinciali L, Santangelo M, Specchio LM, Zaccara G; Epistroke Group. Incidence and predictors of acute symptomatic seizures after stroke. Neurology 2011; 77: 1785-1793.
Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, Cates CU, Creager MA, Fowler SB, Friday G, Hertzberg VS, McIff EB, Moore WS, Panagos PD, Riles TS, Rosenwasser RH, Taylor AJ; American College of Cardiology; American Stroke Association; American Association of Neurological Surgeons; American College of Radiology; American American College of Radiology; Society of NeuroInterventional Surgery; Society for Vascular Medicine; Society for Vascular Surgery. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Circulation 2011; 124: e54-130.
Campbell BCV, Khatri P. Stroke. Lancet 2020; 396: 129-142.
Caplan LR, Hennerici M. Impaired clearance of emboli (washout) is an important link between hypoperfusion, embolism, and ischemic stroke. Arch Neurol 1998; 55: 1475-1482.
Feldman AE, Gidal BE. QTc prolongation by antiepileptic drugs and the risk of torsade de pointes in patients with epilepsy. Epilepsy & Behavior 2013; 26: 421-426.
Fisher RS, Engel JJ Jr. Definition of the postictal state: when does it start and end? Epilepsy Behav 2010;19: 100-104.
GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol 2021; 20: 795-820.
Hart RG, Diener HC, Coutts SB, Easton JD, Granger CB, O'Donnell MJ, Sacco RL, Connolly SJ; Cryptogenic Stroke/ESUS International Working Group. Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol 2014; 13: 429-438.
Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, Kamel H, Kernan WN, Kittner SJ, Leira EC, Lennon O, Meschia JF, Nguyen TN, Pollak PM, Santangeli P, Sharrief AZ, Smith SC Jr, Turan TN, Williams LS. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021; 52: e364-e467.
North American Symptomatic Carotid Endarterectomy Trial Collaborators; Barnett HJM, Taylor DW, Haynes RB, Sackett DL, Peerless SJ, Ferguson GG, Fox AJ, Rankin RN, Hachinski VC, Wiebers DO, Eliasziw M. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med 1991; 325: 445-453.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019; 50: e344-e418.
Saver JL, Carroll JD, Thaler DE, Smalling RW, MacDonald LA, Marks DS, Tirschwell DL; RESPECT Investigators. Long-Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke. N Engl J Med 2017; 377: 1022-1032.
|
