FRONTIERS IN MEDICAL CASE REPORTS - Volume 6; Issue 3, (May-Jun, 2025)
Pages: 01-10
Print Article
Download XML Download PDF
Mifepristone-Induced Hypokalemia Causing Rhabdomyolysis and Severe Acute Kidney Injury: A Case Report
Author: Houtz BL, Newman ED, Cuda TL, Kattel G, Farber JL, Filippone EJ
Category: Medical Case Reports
Abstract:
Mifepristone is a glucocorticoid receptor (GR) blocker approved for improving glucose control in patients with endogenous Cushing’s Syndrome (CS) in whom surgical cure is contraindicated or has failed. Due to GR blockade, levels of ACTH and cortisol become markedly higher. When cortisol levels are sufficiently high, the enzyme conferring aldosterone specificity to the aldosterone-sensitive distal nephron, 11β-hydroxysteroid dehydrogenase type 2, that converts active cortisol to inactive cortisone may be overwhelmed. The result may be enhanced renal potassium excretion and hypokalemia. We report a case of a patient with suspected CS given mifepristone to improve glucose control. The patient subsequently presented with rhabdomyolysis and severe acute kidney injury (AKI) requiring emergency dialysis. Kidney biopsy confirmed myoglobinuria as the cause of the AKI. Despite ongoing cell breakdown, severely reduced GFR, dialysis against a high potassium bath, and daily potassium replacement, the serum potassium took days to normalize. We postulate that mifepristone-induced severe potassium deficiency with hypokalemia was the trigger for rhabdomyolysis and AKI in this patient. This case highlights the vigilance for hypokalemia required when mifepristone is given for improving glucose control.
Keywords: Mifepristone, Cushing’s Syndrome, Rhabdomyolysis, Acute Kidney Injury, Hypokalemia
DOI URL: https://dx.doi.org/10.47746/FMCR.2025.6302
Full Text:
Introduction
A progesterone receptor modulator used as an abortifacient, mifepristone also blocks glucocorticoid receptors (GR) at higher doses. It has been approved for glucose control in adults with endogenous Cushing’s syndrome in whom surgical cure is contraindicated or has failed (Fleseriu et al., 2012). Elevated adrenocorticotrophin hormone (ACTH) and cortisol levels result from GR blockade and cannot be followed as a guide to therapy. A major and well-known side effect of mifepristone is hypokalemia that results from very elevated cortisol levels that overwhelm 11β-hydroxysteroid dehydrogenase-2 (11βHSD2), the enzyme which converts active cortisol to inactive cortisone in the aldosterone sensitive distal nephron (Edwards et al., 1988). Since cortisol has significant affinity for the mineralocorticoid receptor (Funder, 2005), enhanced potassium excretion and hypokalemia may result.
Rhabdomyolysis represents muscle cell necrosis with release of intracellular contents into the circulation, including electrolytes (most notably potassium and phosphorous), enzymes (including creatine kinase, aminotransferases, and lactate dehydrogenase), and myoglobin (Zutt et al., 2014). The latter can cause acute kidney injury and significantly increase the mortality rate. There are multiple causes of rhabdomyolysis, such as trauma, strenuous exertion, limb compression, drugs/toxins, infections, and electrolyte abnormalities, including hypokalemia (Huerta-Alardín et al., 2005).
We present a case of an obese woman with very poor glucose control suspected of having Cushing’s syndrome based on the low-dose overnight dexamethasone suppression test, and who was given mifepristone to improve glucose control. Several months later, she presented with rhabdomyolysis and acute kidney injury (AKI) requiring dialysis. Despite the rhabdomyolysis and severe AKI, the serum potassium on presentation was quite low, a finding that suggested severe hypokalemia from mifepristone was the major cause of the rhabdomyolysis.
Case Presentation
A 76-year-old African American woman with obesity, hypertension, hyperlipidemia, type 2 diabetes mellitus, and chronic kidney disease was suspected to have Cushing’s syndrome because of her obesity and poor glucose control. An overnight low-dose dexamethasone suppression test was positive (8 AM cortisol 2.2 µg/dl), although the diagnosis was not confirmed. Mifepristone was prescribed. Repeat labs after about 2 weeks of receiving mifepristone showed hypokalemia and a bump in creatinine, so spironolactone 25 mg daily was initiated (see Table 1).
Table 1: Relevant Laboratory Values.
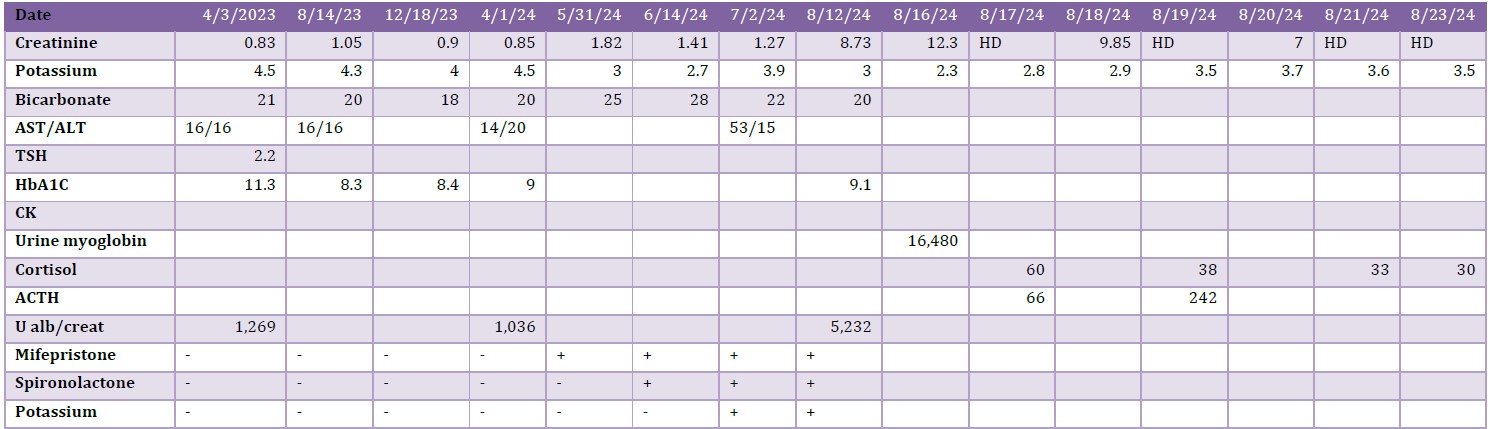
Three weeks later, oral potassium was added to spironolactone for a potassium of 2.7 meq/L. Repeat potassium after another 2 weeks was 3.9 meq/L and creatinine had decreased to 1.27 mg/dl. Repeat labs were next obtained 6 weeks later with a creatinine now of 8.7 mg/dl and potassium of 3.0 meq/L. The patient presented to our hospital emergency department 4 days later with lethargy, nausea, and vomiting with a creatinine of 12.3 mg/dl and a potassium of 2.7 meq/L. Creatine kinase was 2,181 IU/L, TSH 10.53 µIU/ml, and urine myoglobin 16,480 ng/ml. Dialysis was initiated the day after admission for lethargy, anorexia, nausea, and vomiting and continued 3 times/week until discharge, despite remaining non-oliguric. The serum potassium ranged from 2.8 – 3.7 meq/L during the first 5 days despite 3 dialysis treatments with a 4.0 meq/L potassium bath and 200 meq of potassium administered orally. Initial serum cortisol the day after admission was 60 µg/dl (normal: 8 – 10 µg/dl in AM, 2 – 11 µg/dl in PM), slowly declining to 30 µg/dl after 1 week. ACTH was 66 pg/ml (normal: 9 – 46 pg/ml) on day 2 and 242 pg/ml on day 4. Kidney biopsy showed severe acute tubular injury and necrosis with brown pigmented intratubular casts negative for hemoglobin confirming rhabdomyolysis/myoglobinuria as the cause of the AKI (Figures 1 and 2).
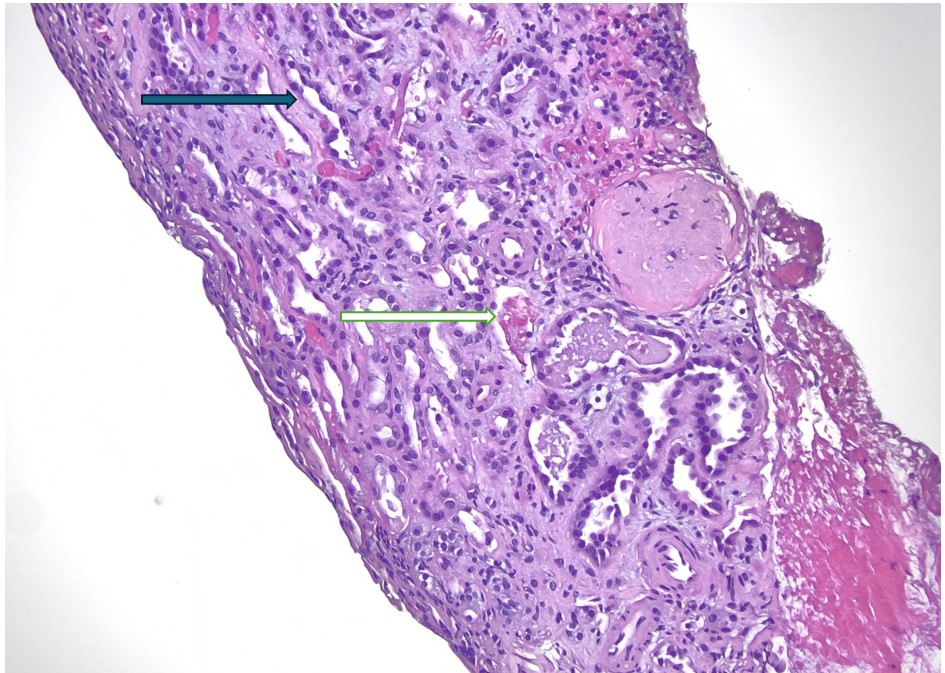
Figure 1: Acute tubular injury and necrosis (black arrow, denuded epithelium) with some tubules showing brownish pigmented casts (white arrow) (H&E; x200).
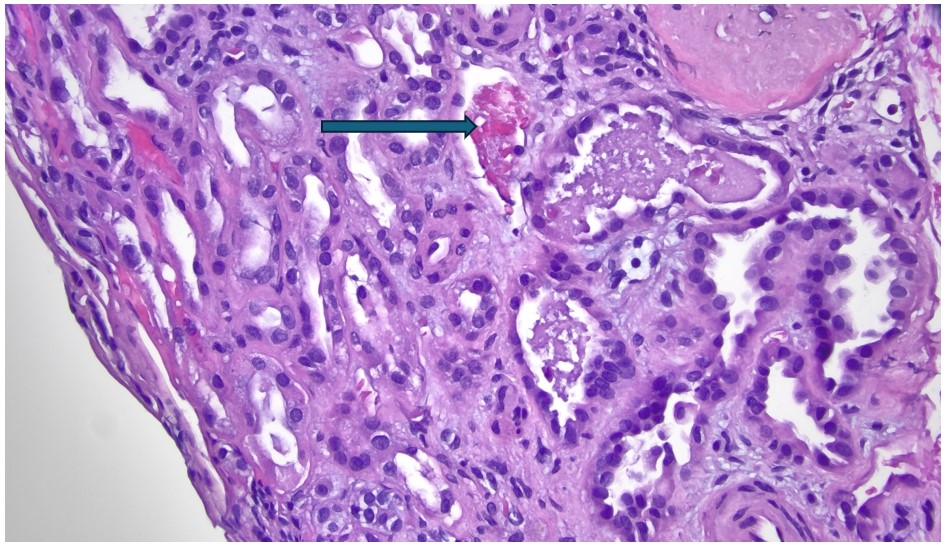
Figure 2: The brownish pigmented casts (arrow) have a granular and beaded appearance (H&E; x400).
Discussion
The optimal therapy for endogenous Cushing’s syndrome is surgical resection of the underlying tumor, be it pituitary, adrenal, or other (Nieman et al., 2015). Medical therapy includes glucocorticoid receptor antagonists, steroid synthesis inhibitors, and anti-pituitary agents (Nieman et al., 2015). The 2012 Study of the Efficacy and Safety of Mifepristone in the Treatment of Endogenous Cushing’s Syndrome (SEISMIC) was an uncontrolled multicenter study of the glucocorticoid receptor antagonist. It was given to 50 patients with endogenous CS and either type 2 diabetes, impaired glucose tolerance, or hypertension. There was a significant improvement in metabolic control (fasting plasma glucose, HbA1C, glucose area-under-the-curve) and blood pressure (Fleseriu et al., 2012). Mifepristone was approved by the FDA in 2012 for control of hyperglycemia in patients with endogenous Cushing’s syndrome with diabetes mellitus or impaired glucose tolerance, who have either failed or are not candidates for surgical cure. In this case report, mifepristone was prescribed by a primary care physician to improve glucose control in an obese patient with suspected Cushing’s syndrome based on a single overnight dexamethasone suppression test.
By inhibiting the glucocorticoid receptor both centrally and peripherally, mifepristone activates the hypothalamic-pituitary-adrenal axis resulting in enhanced release of ACTH and cortisol synthesis (2-fold ACTH increase in 63% of patients and a 7-fold increase in urinary free cortisol in SEISMIC (Fleseriu et al., 2012). Cortisol has significant affinity for the mineralocorticoid receptor at physiologic levels, but it is prevented from activating the receptor in the aldosterone-sensitive distal nephron (late distal convoluted tubule and cortical collecting duct) by conversion to inactive cortisone by 11βHSD2 (Edwards et al., 1988). Hence, mineralocorticoid receptor activation is normally determined by the prevailing aldosterone level, even though orders of magnitude lower than the normal cortisol level. When cortisol is excessively high, as following mifepristone, 11BHSD2 can be overwhelmed and cortisol may activate the mineralocorticoid receptor (Funder, 2005) producing potassium wasting and salt retention (hypertension and edema). Other notable side effects of glucocorticoid receptor blockade include the cortisol withdrawal syndrome from GR blockade (weakness, nausea, headache), endometrial thickening with vaginal bleeding from progesterone receptor modulation, and thyroid function abnormalities (Brown, East et al. 2020).
Hypokalemia is well described with mifepristone. In SEISMIC, 44% of patients had potassium < 3.5 meq/L, including 6% < 2.5 meq/L (Fleseriu, Biller et al. 2012). Corcept Therapeutics, Inc, Menlo ParK CA, a maker of mifepristone (brand name Korlym) that sponsored SEISMIC, convened a panel of endocrinologists to provide consensus recommendations on the use of mifepristone for Cushing’s syndrome (Brown et al., 2020). Hypokalemia was acknowledged as a frequent manifestation. Their algorithm entailed replacing potassium until serum level > 4 meq/L before starting and consideration of proactive spironolactone in all patients beginning 3 – 5 days after mifepristone initiation, dose adjusted for renal function. The potassium level should be checked in 3 – 5 days and at weeks 1 – 2, 4 – 6, and 10 – 12. Significant hypokalemia occurred in our patient even after rhabdomyolysis and severe AKI developed.
Rhabdomyolysis is characterized by a rapid rise of the serum CK to > 5 – 10 times the upper limit of normal, followed by a rapid decline back to normal over days to weeks. This contrasts with chronic or intermittent elevations of creatine kinase, termed hyperCKemia, a much more benign condition from the kidney perspective (Bosch et al., 2009). Clinically, patients with rhabdomyolysis may present with myalgias, weakness, and dark colored urine (Khan, 2009), a triad found in 10% or less of cases. Intracellular contents spill into the circulation, including electrolytes (potassium and phosphate), enzymes (CK, aldolase, transaminases), uric acid, and most notably, myoglobin. Disseminated intravascular coagulation may develop (Danaei et al., 2023). Hepatic dysfunction may also occur, although transaminases may be released from muscle (Lim, 2020). Compartment syndrome may require surgery (Danaei et al., 2023). Acute kidney injury (AKI) is reported to occur in 13% up to 50% of cases (Bosch et al., 2009) and significantly increases mortality.
Multiple causes of rhabdomyolysis exist (Chavez et al., 2016). Trauma (e.g., crush injuries as may occur with major earthquakes) is well-described, but there are multiple other non-traumatic causes: exertion (extreme or moderate in an untrained individual or in adverse circumstances such as extreme heat), ischemia (thrombotic events or prolonged compression/immobilization as occurs with drug overdoses), infections, prescribed drugs (including statins), illicit drugs (cocaine) and alcohol, endocrinopathies (thyroid, diabetes), extremes of temperature (neuroleptic malignant syndrome, serotonin syndrome), and electrolyte abnormalities (hypokalemia, hypophosphatemia).
Several inherited diseases affecting muscle may confer enhanced susceptibility to rhabdomyolysis, including muscular dystrophies, metabolic and mitochondrial myopathies, and congenital myopathies with defective excitation-contraction coupling (Kruijt et al., 2021). An inherited cause should be suspected when rhabdomyolysis is recurrent, there is prolonged hyperCKemia, symptoms of weakness or myalgias are chronic, or family members also have rhabdomyolysis. Kruijt, et al. (2021) retrospectively evaluated 1,302 patients with a CK elevation > 2,000 in a single center and identifies 277 patients (21%) with a presumed underlying genetic neuromuscular cause, 72 of which had a pathogenic variant in a gene increasing susceptibility to rhabdomyolysis. Exercise was the most common trigger (107 cases) among the 277 patients, followed by toxic medications in 55, including 28 on statins, and in 92 multiple triggers were identified. Our patient had no features suggestive of an underlying genetic cause.
Hypokalemia is a well described cause of rhabdomyolysis, including hypokalemia caused by renal potassium wasting from excessive mineralocorticoid receptor activation as occurs with endocrinopathies. Diaz-Lopez et al. published a case report and systematic review through July 2023 totaling 38 cases of primary hyperaldosteronism presenting with hypokalemic induced rhabdomyolysis, including 4 that developed AKI (Díaz-López et al., 2023). All patients were hypertensive and 26 of 38 had serum potassium < 2.0 meq/L with the highest being 2.8 meq/L. Shi, et al. (2024) also presented a case and reviewed the literature through 2023 identifying 43 patients with hypokalemic rhabdomyolysis and primary hyperaldosteronism (incomplete overlap with Diaz-Lopez et al.) of which 33 had serum potassium < 2.0 meq/L and 42 had < 2.5 meq/L. Eight of the 43 developed AKI. Mineralocorticoid receptor activation from an excessively high cortisol level, owing to ectopic ACTH production has also been reported to present with hypokalemic rhabdomyolysis (Qiang et al., 2021).
We posit that mifepristone-induced hypercortisolemia causing hypokalemia is the major reason our patient developed rhabdomyolysis. Statins, including rosuvastatin as our patient was receiving, are well-described causes of rhabdomyolysis (Oshima, 2011). Mifepristone is metabolized by and is an inhibitor of cytochrome CYP3A4, precluding use of statins metabolized by this isoform, such as simvastatin and atorvastatin. As it is metabolized by cytochrome 2C9, rosuvastatin is recommended if a statin is needed in a patient receiving mifepristone. The temporal relationship of the rhabdomyolysis to mifepristone initiation and subsequent hypokalemia supports our contention that hypokalemia was the major trigger for her muscle necrosis, but we cannot exclude the possibility that the statin also had a role (Oshima, 2011).
The mechanism of hypokalemic-induced rhabdomyolysis appears to be multifactorial. Potassium is released from skeletal muscle in response to contraction and results in arteriolar dilatation to enhance muscle blood flow. Knochel and Schlein studied gracilis muscle preparations from normal and potassium deficient dogs and showed significantly reduced muscle blood flow and potassium release from potassium depleted dogs with frank rhabdomyolysis detected in all depleted animals (Knochel and Schlein, 1972). Hypokalemia can increase muscle and liver glycogen storage in the experimental animal (Spergel et al., 1967), but it apparently does not impair glycogenolysis or glycolysis during exercise, at least in the setting of hypokalemic familial periodic paralysis (Engel et al., 1965). Hypokalemia may also disrupt cell membrane ion transport (Shi et al., 2024) by reducing activity of the Na-K-ATPase (Hsu and Guidotti, 1991) with resulting increase in intracellular sodium and subsequently increased intracellular calcium (Lowe et al., 1976), a promoter of rhabdomyolysis.
The pathophysiology of AKI from rhabdomyolysis is multifactorial (Bosch et al., 2009). Myoglobin itself is the main pathogenic culprit, compounded by circulating volume depletion due to sequestration in dying muscle. Three main factors are involved. Firstly, there is preglomerular vasoconstriction that results from activation of renin (and hence angiotensin II), catecholamines, and vasopressin due to a decreased circulating arterial volume. This is compounded by enhanced constricting cytokine production (e.g., endothelin-1, thromboxane A2, tumor necrosis factor-α, etc.) and reduced nitric oxide availability, directly attributable to myoglobin. Secondly, filtered myoglobin may combine with Tamm-Horsfall protein to form casts which obstruct the distal nephron, a process favored by an acidic urine. Finally, myoglobin may be directly toxic to proximal tubular cells by promoting oxidation of released Fe2+ to Fe3+, leading to free radical production. Myoglobin may also result in uncontrolled oxidation of multiple other molecules (Bosch et al., 2009).
The most important therapeutic maneuver to prevent AKI is fluid administration to maximize kidney perfusion, up to one liter/hour as needed especially in crush injuries (Bosch et al., 2009; Gunal et al., 2004). This is most critical during the initial development of muscle necrosis. Saline is preferred but may result in worsening metabolic acidosis from dilution of bicarbonate. Hence, bicarbonate will be needed to prevent or treat acidosis. Whether or not bicarbonate therapy directed at alkalinizing the urine will prevent or ameliorate AKI by reducing myoglobin binding to Tamm-Horsfall protein remains to be proven. Over alkalinization of the urine (pH > 7.5) may be detrimental by inducing calcium phosphate crystallization. Mannitol can also be used to help shrink swollen muscles, enhance the blood volume, scavenge free radicals, and flush out obstructing distal tubular casts. However, no randomized trials have proven a benefit.
Unfortunately, our patient presented one to two weeks after initiation of AKI based on the degree of azotemia precluding aggressive fluid administration as an ameliorating factor. The presentation was typical for rhabdomyolysis as the cause of her AKI given dipstick hematuria in the absence of red cells, low urine sodium, creatinine elevation out of proportion to BUN, and of course, elevated CK and serum/urine myoglobin. However, atypical for rhabdomyolysis was a significantly low potassium, despite cell death in the face of severe AKI, unlike the mild hypokalemia that may be found in some crush victims on presentation (Gunal et al., 2004; Sever et al., 2003). This supports our contention that severe hypokalemia was present before the rhabdomyolysis and was main the initiating factor. Also unusual was the markedly elevated myoglobin despite only mild CK elevations, since the half-life of myoglobin is much shorter than that of CK. In any case, biopsy confirmed myoglobin as the cause of her AKI.
Conclusion
We present a case of severe AKI from rhabdomyolysis following initiation of mifepristone that had significant hypokalemia well after myonecrosis and AKI had occurred. We posit that mifepristone-induced severe hypokalemia was the initial trigger for the rhabdomyolysis, underscoring the close attention that should be paid to the serum potassium following initiation of this drug for CS.
Consent for Publication: Written informed consent obtained from the patient for presenting the case and showing the images and is provided.
Competing Interests: BLH, EDN, TLC, GK, and JLF: none
Edward J Filippone: Speakers bureau for Boehringer-Ingelheim and Lilly, Advisory board for Otsuka
Funding: none
Author Contributions: BLH wrote the first draft. EDN, TLC, GK, JLF, and EJF contributed to writing the final draft. BLH and EJF conceived the idea.
References:
Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med 2009; 361: 62-72.
Brown DR, East HE, Eilerman BS, Gordon MB, King EE, Knecht LA, Salke B, Samson SL, Yuen KCJ, Yau H. Clinical management of patients with Cushing syndrome treated with mifepristone: consensus recommendations. Clin Diabetes Endocrinol 2020; 6: 18.
Chavez LO, Leon M, Einav S, Varon J. Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. Crit Care 2016; 20: 135.
Danaei B, Sharifi A, Mazloom H, Najafi I, Farhang Ranjbar M, Safari S. Prevalence of Compartment Syndrome and Disseminated Intravascular Coagulation following Rhabdomyolysis; a Systematic Review and Meta-Analysis. Arch Acad Emerg Med 2023; 11: e55.
Díaz-López EJ, Villar-Taibo R, Rodriguez-Carnero G, Fernandez-Pombo A, Garcia-Peino R, Blanco-Freire MN, Pena-Dubra A, Prado-Moraña T, Fernández-Xove I, Pérez-Béliz E, Cameselle-Teijeiro JM, Hermida-Ameijeiras A, Martinez-Olmos MA. Should we suspect primary aldosteronism in patients with hypokalaemic rhabdomyolysis? A systematic review. Front Endocrinol (Lausanne) 2023; 14: 1257078.
Edwards CR, Stewart PM, Burt D, Brett L, McIntyre MA, Sutanto WS, de Kloet ER, Monder C. Localisation of 11 beta-hydroxysteroid dehydrogenase--tissue specific protector of the mineralocorticoid receptor. Lancet 1988; 2: 986-989.
Engel AG, Lambert EH, Rosevear JW, Tauxe WN. Clinical And Electromyographic Studies in A Patient with Primary Hypokalemic Periodic Paralysis. Am J Med 1965; 38: 626-640.
Fleseriu M, Biller BM, Findling JW, Molitch ME, Schteingart DE, Gross C; SEISMIC Study Investigators. Mifepristone, a glucocorticoid receptor antagonist, produces clinical and metabolic benefits in patients with Cushing's syndrome. J Clin Endocrinol Metab 2012; 97: 2039-2049.
Funder JW. Mineralocorticoid receptors: distribution and activation. Heart Fail Rev 2005; 10: 15-22.
Gunal AI, Celiker H, Dogukan A, Ozalp G, Kirciman E, Simsekli H, Gunay I, Demircin M, Belhan O, Yildirim MA, Sever MS. Early and vigorous fluid resuscitation prevents acute renal failure in the crush victims of catastrophic earthquakes. J Am Soc Nephrol 2004; 15: 1862-1867.
Hsu YM, Guidotti G. Effects of hypokalemia on the properties and expression of the (Na+,K+)-ATPase of rat skeletal muscle. J Biol Chem 1991; 266: 427-433.
Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis -- an overview for clinicians. Crit Care 2005; 9: 158-169.
Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med 2009; 67: 272-283.
Knochel JP, Schlein EM. On the mechanism of rhabdomyolysis in potassium depletion. J Clin Invest 1972; 51: 1750-1758.
Kruijt N, van den Bersselaar LR, Kamsteeg EJ, Verbeeck W, Snoeck MMJ, Everaerd DS, Abdo WF, Jansen DRM, Erasmus CE, Jungbluth H, Voermans NC. The etiology of rhabdomyolysis: an interaction between genetic susceptibility and external triggers. Eur J Neurol 2021; 28: 647-659.
Lim AK. Abnormal liver function tests associated with severe rhabdomyolysis. World J Gastroenterol 2020; 26: 1020-1028.
Lowe DA, Richardson NP, Taylor P, Donatsch P. Increasing intracellular sodium triggers calcium release from bound pools. Nature 1976; 260: 337-338.
Nieman LK, Biller BM, Findling JW, Murad MH, Newell-Price J, Savage MO, Tabarin A; Endocrine Society. Treatment of Cushing's Syndrome: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2015; 100: 2807-2831.
Oshima Y. Characteristics of drug-associated rhabdomyolysis: analysis of 8,610 cases reported to the U.S. Food and Drug Administration. Intern Med 2011; 50: 845-853.
Qiang W, Song S, Chen T, Wang Z, Feng J, Zhang J, Guo H. A rare case of ectopic ACTH syndrome with rhabdomyolysis. BMC Endocr Disord 2021; 21: 98.
Sever MS, Erek E, Vanholder R, Kantarci G, Yavuz M, Turkmen A, Ergin H, Tulbek MY, Duranay M, Manga G, Sevinir S, Lameire N; Marmara Earthquake Study Group. Serum potassium in the crush syndrome victims of the Marmara disaster. Clin Nephrol 2003; 59: 326-333.
Shi P, Wang C, Lyu Y. Primary aldosteronism with hypokalemic rhabdomyolysis: a case report and review of the literature. J Med Case Rep 2024; 18: 362.
Spergel G, Schmidt P, Stern A, Bleicher SJ. Effects of hypokalemia on carbohydrate and lipid metabolism in the rat. Diabetes 1967; 16: 312-318.
Zutt R, van der Kooi AJ, Linthorst GE, Wanders RJ, de Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord 2014; 24: 651-659.
|
