FRONTIERS IN MEDICAL CASE REPORTS - Volume 3; Issue 4, (Jul-Aug, 2022)
Pages: 1-10
Print Article
Download XML Download PDF
Willis Covered Stent Implantation for Treating Radiation Internal Carotid Blowout Syndrome in Nasopharyngeal Carcinoma
Author: Fangfang Nie, Wu Wang, Peiqiang Yi, Xindong Fan, Weitian Zhang, Xiaojing Yang, Zhen Li, Minghua Li, Chaosu Hu, Xiaomao Guo, Jie Fu
Category: Medical Case Reports
Abstract:
Purpose: The study of Willis covered stent implantation on life-threatening hemorrhage from Radiation Internal Carotid Blowout Syndrome (RICBS) in patients with Nasopharyngeal Cancer (NPC) was evaluated in our hospital. Materials and Methods: Five NPC patients (3 male and 2 female patients) received Willis covered stent implantation from April 2011 to March 2017, in which radiation induced hemorrhage occurred in Internal Carotid Artery (ICA) was included in this study. The median age in the patient cohort was 56 (47-63). All patients were previously treated with radiotherapy (4 received IMRT and 1receivedheavy-ion RT). The median time was four years before the ICA ruptures after irradiation. The RICBS involved the C2 segment of the ICA in three patients and C3 in two patients. Results: All five patients’ ICA bleeding stopped immediately after the operation of Willis covered stent implantation. Follow-up mean time is 10 months. One patient died of suffocation (nasal hematorrhea) 2 weeks after the operation, in which the skull base is involved from recurrent lesions and associated dysphagia. One patient had rehaemorrhagia a week after the operation. One patient died of other accident 15 months after the operation. No adverse effects such as stroke and ischemia were found in all five patients during the follow-up period. Conclusion: The Willis covered stent implantation can immediately stop the bleeding caused by RICBS to save lives immediately. It is an effective and practical method to treat RICBS in NPC patients or other head and neck cancers patients, especially for the radiation-induced vascular events.
Keywords: Willis Covered Stent Implantation, Radiation Internal Carotid Blowout Syndrome, Nasopharyngeal Carcinoma, Head and Neck Cancer
DOI URL: http://dx.doi.org/10.47746/FMCR.2022.3407
Full Text:
Introduction
Radiation internal carotid blowout syndrome (RICBS) is usually unexpected and fatal in head and neck cancer patients. One of the most severe complications is rupture of major vessels, first reported by Thomas and Forbus in 1959. Mortality rates for RICBS have been reported as high as 60%, with neurologic morbidity approaching 40% (Chaloupka et al., 1996). The rate of RICBS in patients receiving salvage head and neck re-irradiation was 2.6%, and the mortality rate was 76% in the McDonald’s study (McDonald et al., 2012). Although the exact mechanism of irradiation-induced vascular pathogenesis is not well established, irradiation is known as the main reason for obliteration of the vasa vasorum, premature atherosclerosis, adventitial fibrosis, and weakening of the arterial wall (Okamura et al., 2002). Irradiation also causes fragmentation of the elastic fibers of the tunica media, subendothelial vascularization and edema (Okamura et al., 2002).
Historically, the RICBS was generally treated with surgical ligation or interventional balloon embolization. Surgery ligation is one of the choices for ICA bleeding as the mortality was 40%-60% (Razack and Sako, 1982) and is potentially associated with post-operation ischemia symptoms. Even though it is characterized by a lower morbidity and mortality rates than surgical procedures, embolization of ICA still presented an unsatisfactory rate of 15-20% rate of developing immediate or delayed cerebral ischemia (Pampana et al., 2011) or diplopia, etc. (Low and Goh, 2003). A possible explanation for this complication involves an incomplete circle of Willis. Hasan (Hasan et al., 2015) suggested that a carotid artery stent graft should be implanted in the early phase before carotid artery hemorrhage.
The Willis covered stent used in our study was developed jointly by our institute and the MicroPort Medical Company. It has been widely used in the cervical artery pseudo-aneurysm, recurrent or primary cystic aneurysm, traumatic aneurysm, and traumatic cervical arterial sinus fistula (Li et al., 2007; Li et al., 2008; Wang et al., 2008; Li et al., 2010a; Zhu et al., 2010; Li et al., 2010b; Tan et al., 2011; Wang et al., 2011a; Wang et al., 2011b). The mechanism of the Willis covered stent involves repairing and rebuilding of the tumor-carrying blood vessels, immediately isolating and blocking the lesions, and keeping the tumor artery open to restore the blood flow of lesions to the normal state. Here we report the application value of the Willis covered stent implantation for radiation ICA bleeding in NPC patients in our study.
Materials and Methods
The Willis Covered Stent
The Willis covered stent was developed by our institute and the MicroPort Medical Company. It is specifically designed for use in the intracranial vasculature and consists of 3 parts: a bare stent, an expandable polytetrafluoroethylene (ePTFE) membrane, and a balloon catheter. Li (Patentee) introduced the structure and application of the Willis covered stent in some other diseases (Li et al., 2007; Li et al., 2008; Wang et al., 2008; Li et al., 2010a; Zhu et al., 2010; Li et al., 2010b; Tan et al., 2011; Wang et al., 2011a; Wang et al., 2011b).
Patients
Five patients (3 male and 2 female patients) with NPC from April 2011 to March 2017 received Willis covered stent implantation, in which the hemorrhage occurred in ICA caused by radiation therapy was involved in this study. The median age of the patients is 57 (47-63). All patients have previously received radiotherapy [4 received IMRT, and 1 received heavy-ion RT]. The median time was performed 4 years (1-8years) before the ICA ruptures after irradiation. All patients with continuous nasal bleeding were confirmed by Digital Subtraction Angiography (DSA). The RICBS involved the C2 segment of the ICA in 3 patients and C3 in 2 patients. Three patients had nasal packing before receiving Willis covered stent implantation but failed, while others did not receive any pretreatment. Once the ICA bleeding was confirmed, all patients received Willis covered stent implantation as emergency treatment. All the patient characteristics are presented in Table 1. Patients received Willis covered stent implantation under local anesthesia. The ICA bleeding is shown in figures (Fig. 1a, Fig. 2a, Fig. 3a, Fig. 4a, Fig. 5a), and the vascular 3D reconstruction of patient 5 was shown in Fig 6. All patients signed the written informed consent form.
Table 1: The information of all patients.

Results
After the covered stent operation, all 5 patients’ ICA bleeding immediately stopped. DSA examination of these 5 patients after operation showed a hemostatic effect of the Willis covered stent implantation (Fig. 1b, Fig. 2b, Fig. 3b, Fig. 4b, Fig. 5b).
The average follow-up time was 7.5 months (0.5-18 months). Patient 1 died 15 months after the operation. Patient 2 died of suffocation (nasal hematorrhea) 2 weeks after the operation with skull base invaded by recurrent lesion and associated dysphagia (posterior cranial nerves symptoms). Patient 5 showed a rehaemorrhagia invasion by tumor a week after operation. No adverse effects such as stroke and ischemia were found in all five patients during the follow-up period.

Figure 1: 1a. Before Willis covered stent implantation (white arrow shows the bleeding site) 1b. After Willis covered stent implantation.

Figure 2: 2a. Before Willis covered stent implantation (white arrow shows the bleeding site) 2b. After Willis covered stent implantation.

Figure 3: 3a. Before Willis covered stent implantation (white arrow shows the bleeding site) 3b. After Willis covered stent implantation.

Figure 4: 4a. Before Willis covered stent implantation (white arrow shows the bleeding site) 4b. After Willis covered stent implantation.

Figure 5: 5a. Before Willis covered stent implantation (white arrow shows the bleeding site) 5b. After Willis covered stent implantation.
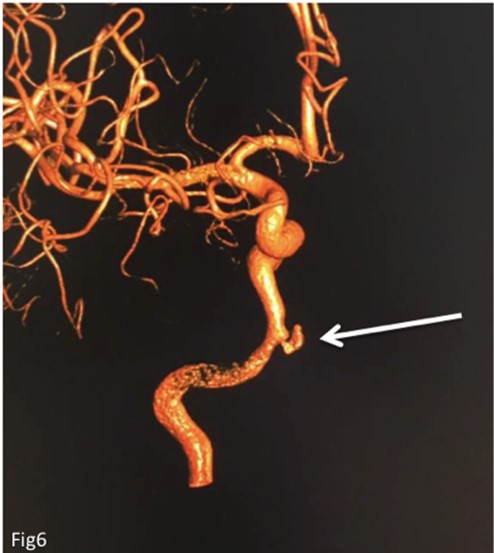
Figure 6: The vascular 3-D reconstruction of patient 5.
Discussion
The morbidity of NPC is 71% of new cases in East Asia and Southeast Asia (Chua et al., 2016). Radiotherapy is considered the preferred radical treatment for NPC and other head and neck cancers. One of the most severe complications is the rupture in major vessels, first reported by Thomas and Forbus in 1959. Mortality rates for RICBS have been reported as high as 60%, with neurologic morbidity approaching 40% (Chaloupka et al., 1996). The rate of RICBS in patients who received salvage head and neck re-irradiation was 2.6% and the mortality rate was 76% in the McDonald’s study (McDonald et al., 2012). The risk of radiotherapy related carotid artery events were analyzed again by Sari (S. Yuce Sari et al., 2016) and Okoye (Okoye et al., 2016) at the 58th American Society for Radiation Oncology (ASTRO) conference in 2016. It is reported that the rate of RICBS was 14% and additional 9 patients (n=132) have succumbed to this complication in Sari’s (S. Yuce Sari et al., 2016) study. RICBS in patients with NPC and other head and neck cancers has existed as an unresolved problem for half a century in the field of radiotherapy. Based on Chaloupka’s (Chaloupka et al., 1996) study, the cause of carotid artery bleeding included tumor invasion, chemotherapy drugs, radiation injury etc. Although the exact mechanism of irradiation-induced vascular pathogenesis is not well established, irradiation is known as the main reason for the obliteration of the vasa vasorum, premature atherosclerosis, adventitial fibrosis, and weakening of the arterial wall (Okamura et al., 2002). Radiation also causes fragmentation of the elastic fibers of the tunica media, subendothelial vascularization and edema (Okamura et al., 2002). Therefore, rupture of irradiated vessels tends to occur in larger arteries that contain the above-mentioned structures and carotid arteries under high blood pressure in the head and neck.
Fletcher indicated that RICBS tended to occur within the first 6 months after therapy (Fletcher and Klein, 1964). However, Okamura et al report two cases of carotid artery rupture with radiation treatment performed 1 year and 17 years ago.
The current treatment for RICBS included surgery ligation and endovascular treatment. Surgery ligation is one of the choices for ICA bleeding because the mortality is 40%-60% (Razack and Sako, 1982) and is potentially associated with post-operation ischemia symptoms. Moreover, tumor invasion or radiation-related anatomic changes increased the difficulty of operation. Endovascular treatment includes balloon or coil embolization, covered stent implantation etc. (Pampana et al., 2011; Low and Goh, 2003; He et al., 2013; Jong et al., 2019). Balloon embolization for carotid artery bleeding was first reported by Osguthorpe (Osguthorpe and Hungerford, 1984) in 1984, and it demonstrated better clinical effects than surgical ligation, as reported by Chaloupka (Chaloupka et al., 1996) in a larger study in 1984. However, the evaluation of Willis’ circle is necessary before ligation or embolization treatment. Even though it is characterized by a lower morbidity and mortality rates than surgical procedures, embolization of ICA still presented an unsatisfactory rate of 15-20% rate of developing immediate or delayed cerebral ischemia (Pampana et al., 2011) or diplopia etc. (Low and Goh, 2003). A possible explanation for this complication could be the incomplete circle of Willis. Therefore, the circle of Willis should be evaluated by angiography before the embolization. The use of covered stents, if possible, minimized the risk of ischemic stroke. By stopping the bleeding and keeping the arterials blood supply, the covered stent implantation could be a good choice for RICBS patients who had underdeveloped circle or patients who has not received the evaluation of Willis’ circle. Implant carotid artery stent graft should be performed in the early phase before the proposal of carotid artery hemorrhage by Hasan (Hasan et al., 2015). However, he did not offer further discussion for existed carotid artery bleeding. The Willis covered stent used in our study was developed jointly by our institute and the MicroPort Medical Company. It has been widely used in the cervical artery pseudo-aneurysm, recurrent or primary cystic aneurysm, traumatic aneurysm and traumatic cervical arterial sinus fistula (Li et al., 2007; Li et al., 2008; Wang et al., 2008; Li et al., 2010a; Zhu et al., 2010; Li et al., 2010b; Tan et al., 2011; Wang et al., 2011a; Wang et al., 2011b). Its mechanism involves repairing and rebuilding of the tumor-carrying blood vessels, immediately isolating and blocking the lesions, and keeping the tumor artery open to restore the blood flow in tumor sites back to the normal state (Li et al., 2007; Li et al., 2008; Wang et al., 2008; Li et al., 2010a; Zhu et al., 2010; Li et al., 2010b; Tan et al., 2011; Wang et al., 2011a; Wang et al., 2011b). Willis covered stent implantation might be a treatment choice of RICBS and good efficacy was achieved with this method. The Willis covered stent implantation achieved good efficacy for radiation ICA bleeding in patients with NPC in our study. In all five of our patients, one single stent was implanted, rather than multiple overlapping stents. The use of extra-long stents in the internal carotid artery has been reported in the literature (Rehman et al., 2017). However, Willis covered stent implantation associated complications such as thrombosis (Liu et al., 2021). Some studies reported unfavorable long-term outcomes after deployment of a foreign body, such as a covered stent, in the field of ongoing contamination and neoplastic disease (Warren et al., 2002; Simental et al., 2003). In our study, one patient died of tumor invasion after Willis covered stent implantation. No other adverse effects such as stroke and ischemia were found in patients. Moreover, stents cannot be successfully implanted in all patients. Stent implantation was treated as the first choice but failed because of moderate lumen stenosis and the emergent massive bleeding in the procedure caused by weak vascular structure, at this moment ICA occlusion can be a choice (Dong et al., 2016). Choi suggested that the protection of ICA during IMRT could decrease the risk of atherosclerosis, and IMRT is still the priority treatment for recurrent head and neck cancer (Choi et al., 2016). Generally, the radiation dose of ICA is higher than 66Gy in primary definitive radiotherapy for NPC, which was confined to gross tumor volume. Moreover, the re-irradiation (>50Gy) is also recommended for the recurrence or metastasis. Sari, et al. (2016) has recently reported that patients whose maximum carotid dose was more than 33Gy and with carotid circumference who received more than 30 Gy was >180° would be at risk of rupture by re-irradiation with stereotactic radiation therapy in recurrent head and neck cancers (S. Yuce Sari et al., 2016). It is used for patients (Wu et al., 2016) who had recurrence after receiving 50Gy heavy-ion radiotherapy, and was diagnosed with bleeding of pseudoaneurysm in ICA after two years. As the most advanced radiotherapy technology, heavy ion radiotherapy may not completely avoid RICBS. We hope that there will be future clinical trials on the mechanism of radiation arterial injury and the implantation of Willis stent-graft to reduce radiation-related vascular complications and provide evidence for the practical treatment of RICBS.
There are some shortcomings in our study. For example, the follow-up time was short, and no longer follow-up was performed. We hope to conduct large-sample, prospective studies in the future.
Conclusions
The Willis covered stent implantation can immediately stop the bleeding caused by RICBS to save patient’s life. It is an effective and practical method to treat RICBS in NPC patients or other head and neck cancer patients, especially in the radiation-induced vascular events.
Acknowledgements: Not applicable.
Conflicts of Interest: The authors declare no conflict of interest.
Author Contributions: FFN, PQY, WTZ analysed the date and wrote the paper. WW, XDF performed the covered stent placement and collected the data. XJY, ZL, JF, MHL, CSH, XMG track the paper. All authors read and approved the final manuscript.
Funding: This work was supported by Hospital Development Center, Shanghai, People’s Republic of China (Grant No. 16CR3112B); Shanghai Sixth People's Hospital Union Project, People’s Republic of China.
References:
Chaloupka JC, Putman CM, Citardi MJ, Ross DA, Sasaki CT. Endovascular therapy for the carotid blowout syndrome in head and neck surgical patients: diagnostic and managerial considerations. AJNR Am J Neuroradiol 1996; 17: 843-852.
Choi HS, Jeong BK, Jeong H, Song JH, Kim JP, Park JJ, Woo SH, Kang KM. Carotid sparing intensity modulated radiotherapy on early glottic cancer: preliminary study. Radiat Oncol J 2016; 34: 26-33
Chua MLK, Wee JTS, Hui EP, Chan ATC. Nasopharyngeal carcinoma. Lancet 2016; 387: 1012-1024.
Dong F, Li Q, Wu J, Zhang M, Zhang G, Li B, Jin K, Min J, Liang W, Chao M. Carotid blowout syndrome after nasopharyngeal carcinoma radiotherapy: successful treatment by internal carotid artery occlusion after stent implantation failure. Springerplus 2016; 5: 1553.
Fletcher GH, Klein R. Dose-time-volume relationship in squamous cell carcinoma of the larynx. Radiology 1964; 82: 1032–1042.
Hasan MM, Sivakumar K, Feuerwerker S. Covered Stents for the Prevention and Treatment of Carotid Blowout Syndrome. BMJ case reports 2015; 77: 164-167.
He CC, Si YF, Xie YA, Yu L. Management of intractable epistaxis in patients who received radiation therapy for nasopharyngeal carcinoma. Eur Arch Otorhinolaryngol 2013; 270: 2763-2767.
Jong MA, Candanedo C, Gross M, Cohen JE. Intervening in the Acute Phase of Postradiation Carotid Blowout Syndrome. Int Arch Otorhinolaryngol 2019; 23: 172-177.
Li MH, Leng B, Li YD, Tan HQ, Wang W, Song DL, Tian YL. Comparative study of covered stent with coil embolization in the treatment of cranial internal carotid artery aneurysm: a nonrandomized prospective trial. Eur Radiol 2010a; 20: 2732-2739.
Li MH, Li YD, Gao BL, Fang C, Luo QY, Cheng YS, Xie ZY, Wang YL, Zhao JG, Li Y, Wang W, Zhang BL, Li M. A new covered stent designed for intracranial vasculature: application in the management of pseudoaneurysms of the cranial internal carotid artery. AJNR Am J Neuroradiol 2007; 28: 1579-1585.
Li MH, Zhu YQ, Fang C, Wang W, Zhang PL, Cheng YS, Tan HQ, Wang JB. The feasibility and efficacy of treatment with a Willis covered stent in recurrent intracranial aneurysms after coiling. AJNR Am J Neuroradiol 2008; 29: 1395-1400.
Li YD, Li MH, Gao BL, Fang C, Cheng YS, Wang W, Li WB, Zhao JG, Zhang PL, Wang J, Li M. Endovascular treatment of recurrent intracranial aneurysms with re-coiling or covered stents. J Neurol Neurosurg Psychiatry 2010b; 81: 74-79.
Liu C, Shen Y, Qian K, Hu Y, Hu X, Wu X. Application of covered stent graft in the treatment of complex carotid artery lesions: A single center experience. Vascular 2021; 28: 17085381211040991.
Low YM, Goh YH. Endovascular treatment of epistaxis in patients irradiated for nasopharyngeal carcinoma. Clin Otolaryngol Allied Sci 2003; 28: 244-247.
McDonald MW, Moore MG, Johnstone PA. Risk of carotid blowout after reirradiation of the head and neck: a systematic review. Int J Radiat Oncol Biol Phys 2012; 82: 1083-1089.
Okamura HO, Kamiyama R, Takiguchi Y, Kimizuka K, Ishikawa N, Kishimoto S. Histopathological examination of ruptured carotid artery after irradiation. ORL J Otorhinolaryngol Relat Spec 2002; 64: 226-228.
Okoye CC, Zheng Y, Muzic RF, Yao M, Dorth JA. Imaging Treatment-Related Carotid Artery Inflammation in Head and Neck Cancer. Int J Radiat Oncol Biol Phys 2016; 94: 927-927.
Osguthorpe JD, Hungerford GD. Transarterial carotid occlusion. Case report and review of the literature. Arch Otolaryngol 1984; 110: 694-696.
Pampana E, Gandini R, Stefanini M, Fabiano S, Chiaravalloti A, Morosetti D, Spano S, Simonetti G. Coronaric stent-graft deployment in the treatment of carotid blowout. Interv Neuroradiol 2011; 17: 490-494.
Razack MS, Sako K. Carotid artery hemorrhage and ligation in head and neck cancer. J Surg Oncol 1982; 19: 189-192.
Rehman AA, Turner RC, Lucke-Wold BP, Boo S. Successful Treatment of Symptomatic Intracranial Carotid Artery Stenosis Using a 24-mm Long Bare Metal Coronary Stent. World Neurosurg 2017; 102: 693.e15-693.
S. Yuce Sari MC, Yazici G, Ozyigit G, Kivanc H, Yildiz D, Yildiz F, Akyol F, Zorlu F, Gurkaynak M. Results of Reirradiation with Stereotactic Radiation Therapy in Recurrent Head and Neck Cancer. 58th ASTRO 2016 Radiation Oncology Annual Meeting, Boston, USA 2016: Poster No.1131.
Simental A, Johnson JT, Horowitz M. Delayed complications of endovascular stenting for carotid blowout. Am J Otolaryngol 2003; 24: 417-419.
Tan HQ, Li MH, Zhang PL, Li YD, Wang JB, Zhu YQ, Wang W. Reconstructive endovascular treatment of intracranial aneurysms with the Willis covered stent: medium-term clinical and angiographic follow-up. J Neurosurg 2011; 114: 1014-1020.
Thomas E, Forbus WD. Irradiation injury to the aorta and the lung. AMA Arch Pathol 1959; 67: 256-263.
Wang JB, Li MH, Fang C, Wang W, Cheng YS, Zhang PL, Du ZY, Wang J. Endovascular treatment of giant intracranial aneurysms with willis covered stents: technical case report. Neurosurgery 2008; 62: E1176-E1177.
Wang W, Li MH, Li YD, Gu BX, Wang J, Zhang PL, Li M. Treatment of traumatic internal carotid artery pseudoaneurysms with the Willis covered stent: a prospective study. J Trauma 2011a; 70: 816-22.
Wang W, Li YD, Li MH, Tan HQ, Gu BX, Wang J, Zhang PL. Endovascular treatment of post-traumatic direct carotid-cavernous fistulas: A single-center experience. J Clin Neurosci 2011b; 18: 24-28.
Warren FM, Cohen JI, Nesbit GM, Barnwell SL, Wax MK, Andersen PE. Management of carotid 'blowout' with endovascular stent grafts. Laryngoscope 2002; 112: 428-433.
Wu CJ, Lin WC, Hsu JS, Han IT, Hsieh TJ, Liu GC, Chiang IC. Follow-up for covered stent treatment of carotid blow-out syndrome in patients with head and neck cancer. Br J Radiol 2016; 89: 20150136.
Zhu YQ, Li MH, Fang C, Tan HQ, Wang W, Zhang PL, Cheng YS, Wang JB, Ma LT. Application of the Willis covered stent in the treatment of aneurysm in the cisternal segment of the internal carotid artery: a pilot comparative study with midterm follow-up. J Endovasc Ther 2010; 17: 55-65.
|
